
Neil Versel has a good story this week on Mobihealthnews about competition among tablet manufacturers for the health care market. He notes the considerable potential market demand for tablet computers with the right features and capabilities.
It is true the iPad is magical. Don't deny that. On the other hand, there seems to be a lot of Apple fan-boy hyperbole surrounding the iPad in health care. Most stories on the iPad in health care focus on what a sexy product it is and how clinicians would love to use it in their practice. But there's more to gaining market share in health care than a sexy product with usability and customer hopes, wishes and desires.
There are 4 key hurdles any tablet manufacturer must overcome to succeed in health care. First, software developers must redesign the user interface of their applications to run on the smaller screens of tablets (compared to desk top computers). This is no easy task, but at HIMSS last month, it seemed everyone had (or promised have soon) demo software running on the iPad. A great tablet that no one's ever heard of, from Emano Tec, faded away at least partially due to a lack of applications designed for it's form factor. And it is not clear that HIT vendors will jump at the chance to re-implement their software on multiple tablets, let alone the iPad.
The next hurdle is that deploying IT infrastructure in hospitals is not a consumer play. Due to HIPAA and other requirements, providers need a device with complete and robust enterprise features. Centralized provisioning and device management, authentication, strong encryption, and top notch wireless performance are required for broad cost effective deployment in health care. This is not currently an iPad strength.
Many caregivers work 12 hour shifts, and all tablet users will need both long battery life (ideally lasting a full shift). Once the battery is depleted, it needs to be recharged -- in a commercial grade, ganged charger (i.e., one that charges multiple devices at once). Installing a bunch of power strips on a counter and plugging in wall warts that then attache to individual tablets consume too much space, are a hassle to use and manage, and represent an infection control risk. There may be tablets that meet the battery life requirement, but none offer ganged charging stations.
Finally, tablets used at the point of care require certain physical characteristics. While office based physicians may be able to get by without some of these requirements (like infection control and disinfecting devices used at the point of care), they are a necessity for hospitals. The first requirement is ruggedization and the ability to be dropped repeatedly onto linoleum covered concrete from 1 meter. Second is water resistance, to both patient fluids and when the tablet is wiped down with disinfectants. And tablets must be made out of materials that are not susceptible to the effects of the harsh disinfectants used in health care. A common problem with products used at the point of care and exposed to disinfectants over time is brittleness resulting in cracking and breaking of cases and parts exposed on the outside of devices.
After-market cases are available to overcome some or all the physical limitations of current tablets, especially ruggedization and water resistance. But these cases come at a cost - they increase the size and weight of the device, and may impact the the use of speakers and microphone, visibility of the display and touch screen performance.
Presently none of the tablets on the market meet all the requirements for health care. Most probably don't meet any of them without a third party case.
So what are today's tablets really capable of in health care? Sales demos and pilot deployments. [See update below.]
Over time, I expect tablets to evolve much like VoIP handsets. The initial versions of handsets sold into health care were designed for corporate suites. But over time, they became ruggedized, water resistant, and manufacturers changed to materials that could withstand the disinfectants used in health care. I suspect that manufacturers who primarily target commercial markets, rather than the consumer market, will be the first to adopt these industrial-type requirements. I also suspect that there are more tablets to come from other vendors in the enterprise telecom or Unified Communications markets.
If Apple wants the iPad to dominate in health care (and that seems to be an open question at this time), they'll have to step up, and do it in a timely fashion. It would seem that a platform OS like Android, that runs on multiple manufacturers' tablets would be a very attractive feature to most HIT vendors. I'm sure the HIT vendors are hoping to port their software to one tablet OS, rather than 2 or 3.
It's a wide open market, with lots of customer demand - and at this point I wouldn't count anyone out.
UPDATE: It strikes me that I should say more about the short term prospects of the iPad in health care. Sales demos are an application with significant potential; iPads are sexy and attractive and would likely enhance almost any application's demo. Pilots are undertaken by early innovator customers. These are the folks who are willing to give up features that are essential to early and late majority buyers - like the shortcomings in the 4 categories above. I suspect that early innovators will enthusiastically embrace iPads. But early innovators does not a successful market make. Using Geoffry Moore's market development model, the iPad or any tablet needs a whole product solution (again the 4 categories above) before it can cross the chasm to the majority of the market. A market limited to just the early innovators is likely to be ten percent or less of the total market opportunity.
Here are photos of some of the tablets at HIMSS11 in Orlando.
-

- AirStrip application on iPhone and iPad

-

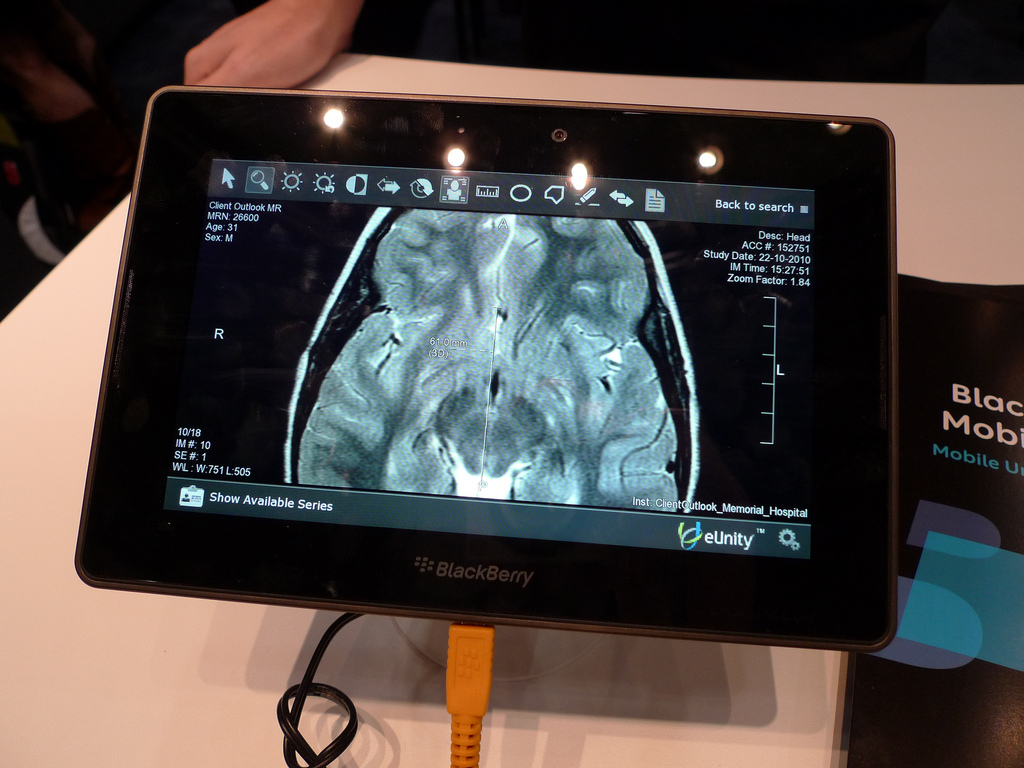
- BlackBerry Playbook tablet
-

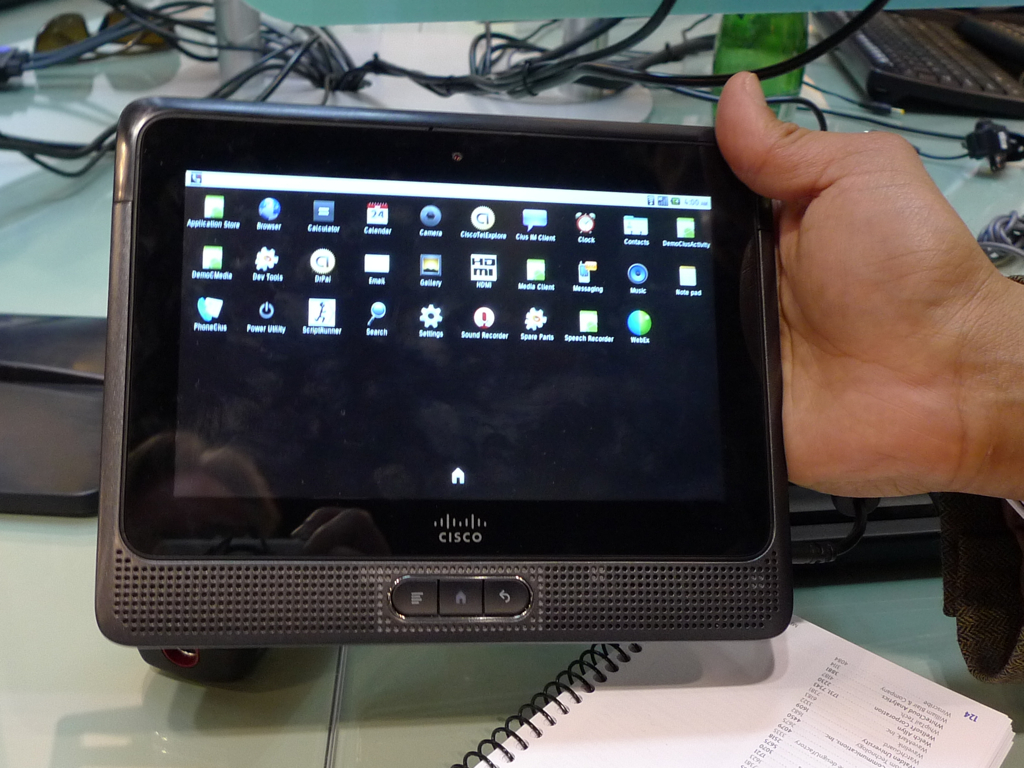
- Cisco Ceeus tablet
-

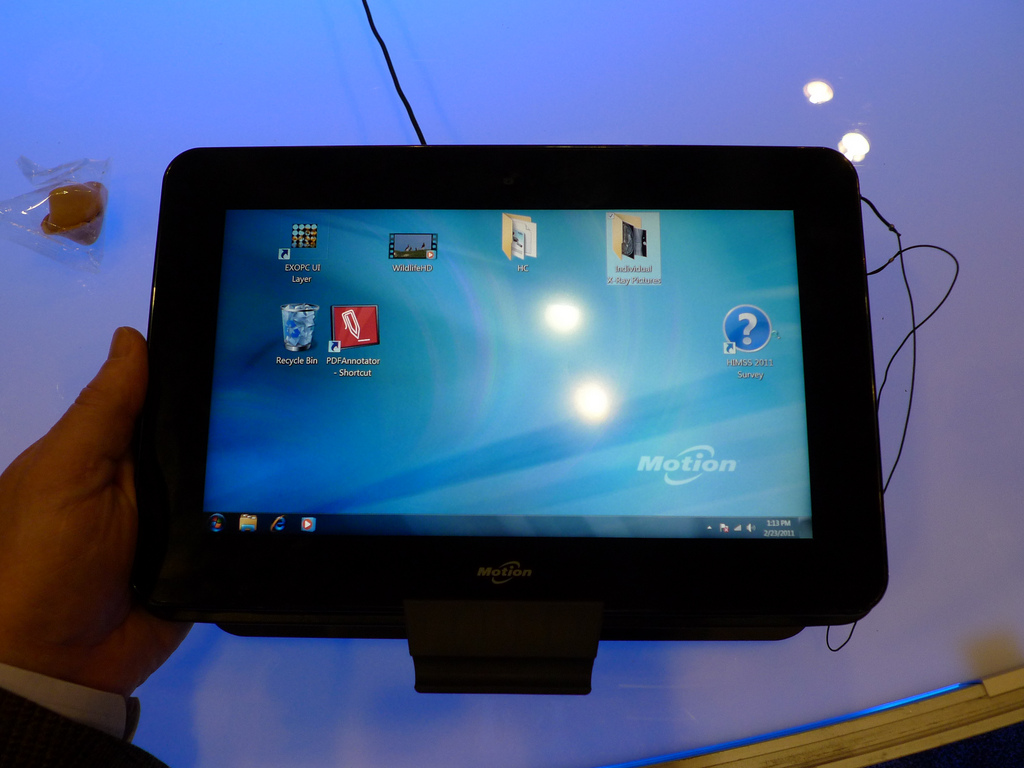
- Motion CL900 tablet
UPDATE: I missed the Avaya Flare.
[thumbnail photo source: The Economist, via iPhoneIndiaBlog.com]


Great points about the iPad in the healthcare setting - reminds me of the dead COW analogy. I was doing some work in a hospital last year and during the walk-through they said they were getting rid of COWs and moving to fixed computers in all patient rooms - they had wireless dead-spot issues and battery issues (one doctor took to carrying his own battery!). If the iPad is anything like my iPod Touch, ouch - battery power length is next to non-existent in ‘shift-like’ terms. AND, the clinicians will expect high fidelity with the iPads as they check on YouTube, stocks, etc…and the virtual environment running the EHR app.
The early adopters are great for hype, but it’s the manufacturers who stay for the long-run and fix the issues that end up with most of the market share.