
I wrote in the beginning of 2012 that perhaps that year was the year for mHealth to ‘breakout. ‘ I cited several proclamations and organizational activities to support that claim. mHealth and the use of remote monitoring as an integrated healthcare offering is still not as prevalent as one would think it would be two years later. Even in the Telemedicine & E-Health LinkedIn Group, one sees angst at the low adoption rate of the use of telehealth solutions. Inevitably, when I speak with my colleagues and other people involved in healthcare, economic and clinical effectiveness questions prevail. Two specific conversations I had with clinicians stand out. In one, the cardiologist had not seen enough evidence that the quality of care and cost would justify a large addition or change to the existing healthcare offerings. In another, the clinician reminded me that with chronic diseases, one is attempting to get patients to change their behavior, which is very difficult, regardless of any technology involved.
With the above in mind, I’d like to offer the following results from the Renewing Health (RH) project in Europe, a randomized control trial which endeavored to compare the use of remote monitoring technologies and workflows with traditional workflows in the management of chronic disease in both economic and clinical terms. While the final results of the whole study are due out this summer, Veneto, Italy, has presented their findings for congestive heart failure (CHF) and they are fairly impressive.
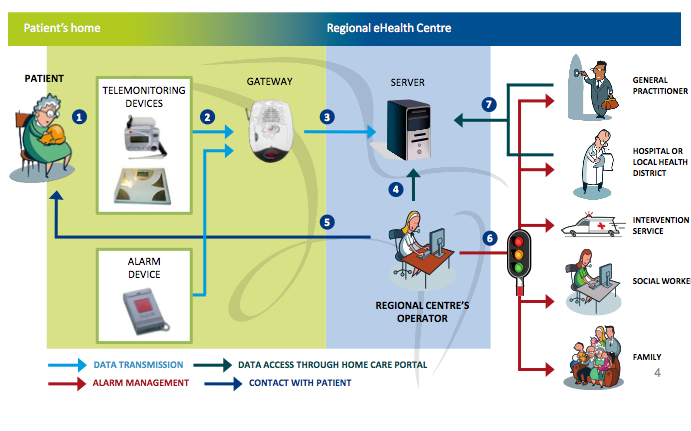
Veneto, Italy, had to redesign their clinical workflow to accommodate a telehealth center which functioned as a data aggregation, filtering and analysis point for the data flowing from a patient home. This telehealth center then interacted with the patient, emergency services and clinical personnel based on a set of ‘clinical rules’ regarding the data received. This helped to alleviate data overflow and false alarms sent to the clinician and only ‘actionable’ information was forwarded when clinical intervention was needed. This also helped to gain the trust of all parties in the study; patients felt they were being monitored appropriately; clinicians were notified when it was truly necessary for them to intervene, and yet they could retrospectively review the data if required; and, emergency services were called appropriately and also were able to retrospectively review data if necessary.
After adopting this architecture and workflow, Veneto, Italy had the following results from their pilot study. Economically, their traditional healthcare model cost 4.72 Euro per day, whereas the remote monitoring healthcare model cost 3.47 Euro per day for a cost reduction of 16.5%. The clinical outcomes really improved with a 35% reduction in CHF hospital admissions, a 42% reduction in the number of specialist visits for CHF and a 32% reduction in specialist procedures for CHF. These are excellent results and Veneto will be using this model as their standard of care for future management of CHF patients. One of the main keys to attaining these results was the re-engineering of their workflow architecture to include the telehealth center in the middle of the data flow. For a more detailed view of these results, you may go here.
Additionally, the RH results will be forthcoming regarding Diabetes and Chronic Obstructive Pulmonary Disease (COPD). A follow-on project which is studying remote monitoring for chronic diseases called United4Health is requiring a standard system architecture of the pilot sites as well as ensuring remote monitoring workflows are part of the standard of care for the pilot site. It is not a randomized control trial, so the power of the results as compared to RH will probably not be as high, however, the insistence that the remote monitoring workflow be a part of the offered services and not a ‘one-off’ will be of value for the study of the ‘normalization’ of remote monitoring technologies in the standard of care for chronic diseases.
To contrast, the results above from RH are in complete contradiction to the general results from the Whole System Demonstrator (WSD) Project which finished up in early 2013. The conclusion of that study stated that “Telehealth does not seem to be a cost effective addition to standard support and treatment.” To be fair the WSD results were for all three chronic diseases of CHF, Diabetes and COPD. It remains to be seen if the RH combined results will be similar. Nevertheless, for CHF, it seems as though remote monitoring can be a better approach both clinically and economically for disease management as long as the system architecture and clinical workflows are designed to facilitate the proper interventions.
As an aside, from a clinical engineering viewpoint, it is interesting to note that Veneto outsourced both the telehealth center and home monitoring functions. If you drew a vertical line at the output of the telehealth center, that would be where the Veneto healthcare organizations interfaced with the rest of the remote monitoring architecture. With other pilot sites, they only outsourced the home monitoring function, so the healthcare organization provided the telehealth center functions of aggregating, filtering and analyzing the remote monitoring data. This interface point and function decision is important in the context of what parts of the telecommunication and function infrastructure does your healthcare enterprise wish to control and is a prime example of what was discussed in the previous blog post on mHealth.
Disclaimer, I am involved in the Renewing Health (RH) and United4Health projects as a technical manager of the industry advisory board. In that role, I worked with the pilot sites to document their system architectures and identify any issues with which industry could assist them. You can find details in the system architectures and technical issues at both the beginning and end of the RH study here. United4Health is in its beginning stages and the public documents have not yet been released. Nevertheless, the website listed above will contain those documents as they are released over the length of the study.


{kind=link}
Recent Comments