Ranking the Importance of SaMD — Software as a Medical Device (UPDATE)
In the May 10th Pre-Cert webinar the FDA addressed an interesting risk matrix that was previously...
Read More

In the May 10th Pre-Cert webinar the FDA addressed an interesting risk matrix that was previously...
Read More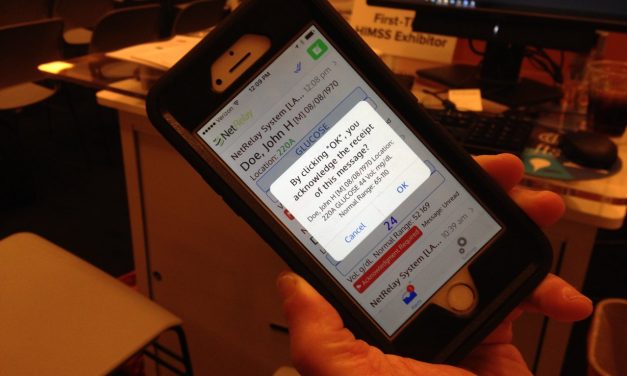
In this post we will delve into a growing enterprise software category, health care messaging...
Read More
Two years ago, I was at eHealth week in Athens, Greece, and stumbled upon several other Americans...
Read More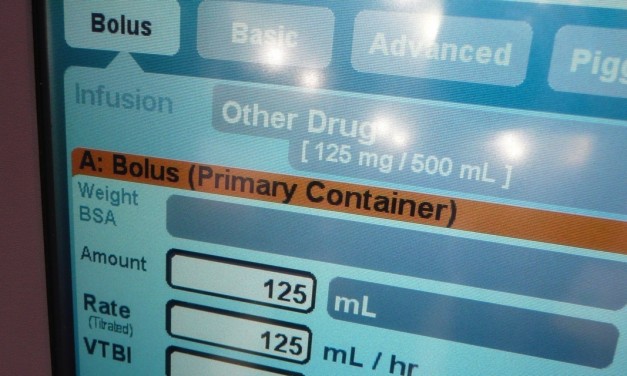
It is somewhat ironic that Hospira and Cerner announced a new collaboration on Hospira’s infusion...
Read More
The Office of the Inspector General (OIG) of the U.S Department of Health and Human Services has...
Read More
This summer, FDA proposed lifting regulations from certain currently regulated medical devices....
Read More
The previous post in this series suggested a set of characteristics to define the messaging...
Read MoreThe recent recall (links below) for McKesson’s Anesthesia Care system raises interesting questions about potential information system failure modes as well as what system/software functions cross the imaginary line between...
Read More
On a recent LinkedIn group discussion, the following question was posed by Taimoore (Tim) Rajah of...
Read MoreSome time ago Tim Gee pointed out that a major vendor for an in hospital communication system included the following statement in its documentation: "This product is not intended for use with patient monitoring devices or other...
Read MoreOn September 4, 2013, the FDASIA mandated workgroup presented their recommendations to the Health IT Policy Committee in Washington, D.C. Some reporting on the meeting cast the draft report as downplaying potential FDA...
Read MoreA while back I was provided with a review copy of the book, Electronic Health Record: A Systems Analysis of the Medication Domain, by Alexander Scarlat, MD. This book is intended to serve as a practical book about electronic...
Read More
As noted before, from time to time I answer questions and exchange ideas with folks from...
Read MoreLast month I spoke at the first CIS Qatar International Conference in Doha Qatar. My topic was the Importance of Enterprise Wide Medical Device Integration in CIS workflow. You can download a copy of my presentation here. This...
Read MoreIn preparing for my presentation on Stage 2 Meaningful Use (MU) requirements for the November, 2012 Fourth Annual Medical Connectivity Conference I had the opportunity to delve further into the question of what had to be...
Read More

Recent Comments