How to Eliminate Innovation Obstacles
Innovation — whether in business, technology or health care delivery — is about figuring out how...
Read More
Innovation — whether in business, technology or health care delivery — is about figuring out how...
Read More
The method of arranging medical devices and those that recognize and respond to alarms is...
Read More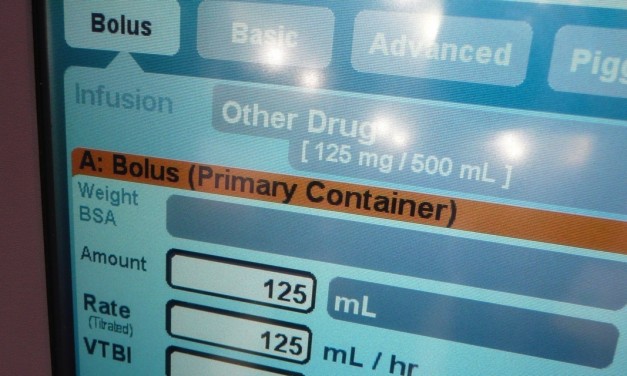
It is somewhat ironic that Hospira and Cerner announced a new collaboration on Hospira’s infusion...
Read More
This summer, FDA proposed lifting regulations from certain currently regulated medical devices....
Read More
Clinical alarm safety can be hard to achieve, and once attained, a struggle to maintain. There are...
Read More
Challenges with alarm notification and fatigue have plagued the health care industry for decades....
Read MoreExcept for emergent situations, no medical device is used without an order. And if not an order written to accomplish a certain clinical task for a specific patient, then "standing" orders captured in written policies and...
Read MoreScheduling is not a workflow one normally associates with medical device connectivity. In some applications, scheduling is handled by software separate from the connectivity solution. Sometimes, scheduling is not done at all. In...
Read MoreConnectivity enabled medical devices send patient data right out of the medical device to a network, be it a body area network, cellular broadband network, home or enterprise network. The network then conveys this medical device...
Read MoreOn April 8, 2013, the Joint Commission published a Sentinel Event Alert on medical device alarm safety in hospitals. Once again, alarm hazards tops the ECRI Institute's 2013 Top 10 Health Technology Hazards. Alarm fatigue is...
Read MoreA recent Class I recall (not pictured) of a medical monitor with a hospital network connected central station stimulates some generalities about software, "fixes", and connectivity. (Class I recalls are defined by the FDA as a...
Read MoreThe issue of the EHR relative to safety and effectiveness has again made the news with the November 7, 2011 pre-publication (and downloadable) release of an Institute of Medicine report on EHR safety, commissioned by the U.S....
Read MoreLet’s always pause long enough to do some risk management thinking…
Read MoreThere are very few instances of IV pump connectivity to EMR or alarm systems.
Read More
The ability to support third party apps on a PC that’s a medical device is highly dependent on the design approach and verification testing used by the manufacturer.
Read More

Recent Comments