Capsule Tech Acquires Bernoulli Health: Analysis
On April 30, 2019, Capsule Tech announced that it is acquiring Bernoulli Health for an undisclosed...
Read More

On April 30, 2019, Capsule Tech announced that it is acquiring Bernoulli Health for an undisclosed...
Read MoreThis post details the medical device directory I built demonstrating the concept of a knowledge...
Read MoreOverview of Medical Device Integration Task I provided an overview of integrating medical device systems and information into an EHR in a paper I wrote in 2008. The figure below provides a graphical representation of the...
Read More
While reading a couple of articles in the healthcare IT industry, several statements stood out as...
Read More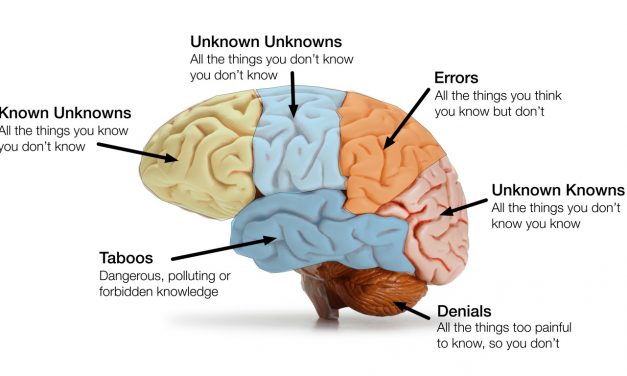
Innovation — whether in business, technology or health care delivery — is about figuring out how...
Read More
The business delivery system (BDS) for a company includes all of the operational resources,...
Read More
The Office of the Inspector General (OIG) of the U.S Department of Health and Human Services has...
Read More
This summer, FDA proposed lifting regulations from certain currently regulated medical devices....
Read More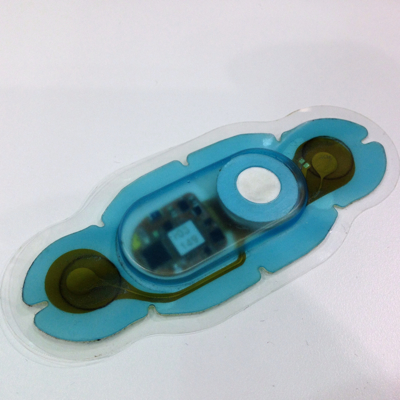
I was listening today to the CE-IT Webinar on CE and HIT from the 2014 AAMI conference in...
Read MoreExcept for emergent situations, no medical device is used without an order. And if not an order written to accomplish a certain clinical task for a specific patient, then "standing" orders captured in written policies and...
Read MoreScheduling is not a workflow one normally associates with medical device connectivity. In some applications, scheduling is handled by software separate from the connectivity solution. Sometimes, scheduling is not done at all. In...
Read MoreConnectivity enabled medical devices send patient data right out of the medical device to a network, be it a body area network, cellular broadband network, home or enterprise network. The network then conveys this medical device...
Read MoreA key feature of all connectivity solutions is a database that includes all of the patients associated with the system's medical devices. This is called a "patient census" or ADT (admission, transfer and discharge), much like...
Read More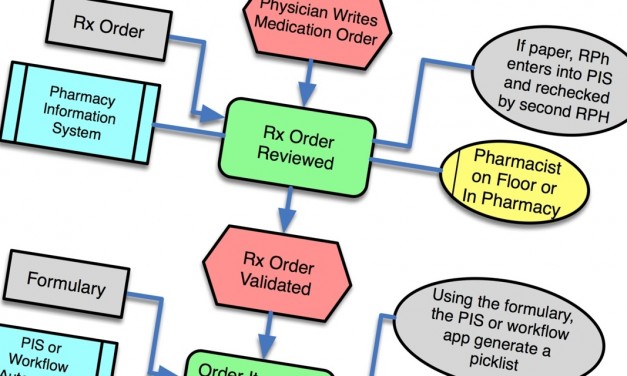
One of the biggest challenges for medical device makers developing connectivity solutions is to...
Read More
Creating and launching innovative ground-breaking new technologies and solutions is a heady...
Read More

Recent Comments