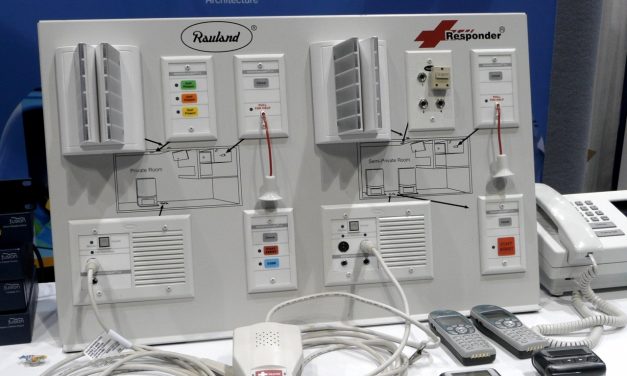
Disrupting Nurse Call
Change is disrupting nurse call. After decades of slow incremental change, the pace of change is...
Read More
Change is disrupting nurse call. After decades of slow incremental change, the pace of change is...
Read More
On April 30, 2019, Capsule Tech announced that it is acquiring Bernoulli Health for an undisclosed...
Read More
Hill-Rom announced March 12, 2019 that it was in the process of acquiring Voalte for $180 million....
Read More
In June 2018 the FDA released an update to its working model of the Software Precertification...
Read More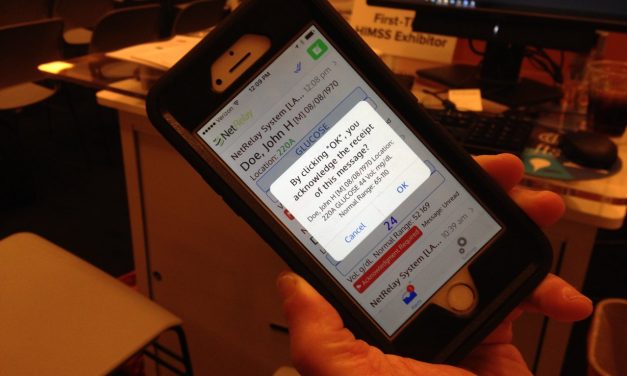
In this post we will delve into a growing enterprise software category, health care messaging...
Read More
In the cottage industry that is health care, there are many interstitial spaces between health...
Read More
Innovation — whether in business, technology or health care delivery — is about figuring out how...
Read More
The business delivery system (BDS) for a company includes all of the operational resources,...
Read More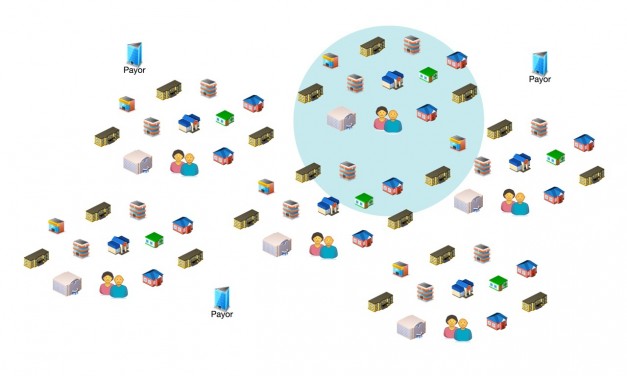
As a $1.7 trillion market with $3.24 trillion in health care expenditures in 2015, the US health...
Read More
I was listening today to the CE-IT Webinar on CE and HIT from the 2014 AAMI conference in...
Read More
The previous post in this series suggested a set of characteristics to define the messaging...
Read More
What do secure communications, care team coordination, patient engagement various workflow...
Read More
It's useful to segment and analyze markets for developing company and product strategy or...
Read More
The above title is the topic for my presentation at this year's Medical Device Connectivity...
Read More
As noted before, from time to time I answer questions and exchange ideas with folks from...
Read More

Recent Comments